best weight loss surgery, plastic surgery, cosmetic surgery, gastric sleeve, gastric bypass, gastric mini bypass, hair transplant, dental treatments, implants , in turkey. Affordable, safe, satisfactory results.
best gastric sleeve surgeon, best plastic surgeon, most safe weight lost hospital in turkey.
Renovated Me
BLOG POSTS
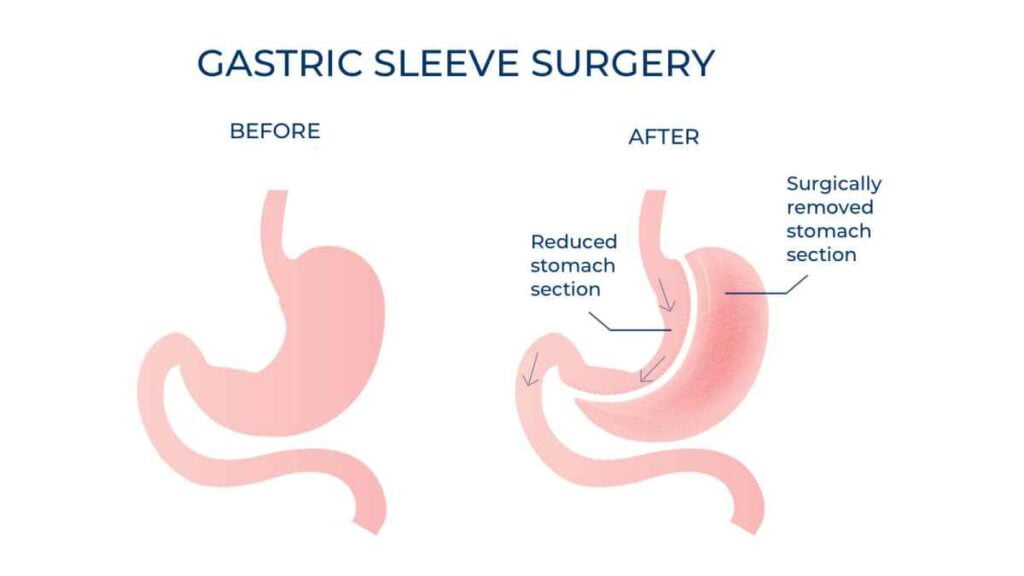
What is Gastric Sleeve - Sleeve Gastrectomy?
Laparoscopic Sleeve Gastrectomy (LSG), was first conceived as a first step of a two staged procedure that included a duodenal switch in 2000 (and later Roux-en-Y gastric bypass), and popularized by Dr. M. Gagner. (1) Subsequently, with the use of smaller bougies, the operation was adopted as a primary procedure. Over time the LSG has become the most popular bariatric operation world wide. Most studies have demonstrated that the LSG is effective for weight loss and results in improvement and even resolution of co-morbidities like type 2 diabetes, quite similar to Roux-en-Y gastric bypass, but with less morbidity, and mortality.
Need more information about surgeries?
For more information about our you can contact us and get more details.

Procedure
The operation is commenced by using energy devices to take down the greater curvature of the stomach from the antrum to the Angle of His. This includes dividing various branches of the gastroepiploic vessels, close to the gastric wall of the greater curvature. Most operators will fully mobilized the fundus posteriorly, lysing the adhesions in the lesser sac and anterior to the pancreas (more so behind the antrum). The left crus is also exposed to investigate the presence of a hiatal hernia. Most surgeons will selectively close hiatal hernias when identified. Some surgeons will also mobilize the fat pad near the gastro-esophageal junction to better identify this area and staple accordingly. A bougie is introduced trans orally (32-40Fr) and positioned abutting the lesser curvature. The stapling begins 1-6 cm proximal to the pylorus and aiming lateral to the bougie. Strictures are avoided at the incisura angularis by avoiding stapling too close (or tight) to the bougie. One also has to avoid stapling the esophagus near the GE junction, as most leaks occur distal or near the GE junction. Choosing the appropriate staple height depends on gastric tissue thickness and varies according to the sex, BMI and stomach site. Wall thickness tends to decrease from distal to proximal. Appropriate compression time is necessary, especially in thick tissue. Most surgeons will reinforce the staple line in order to decrease bleeding and leaks. Reinforcement options include suturing or buttressing. Drainage and leak testing is left to the discretion of the surgeon.
Outcomes
Like the Roux-en-Y gastric bypass, most of the weight loss is achieved in the first 2 years (>70% excess weight loss for BMI less than 50). Weight regain and gastric pouch dilatation can be seen thereafter. At 5 years, there is a sustained weight loss in the range of 50-60% of excess weight.
For super-obese patients, a two-stage approach (LSG first followed by completion to a duodenal switch or gastric bypass) has decreased mortality and morbidity from procedures done in one stage. The most feared complication of the LSG is gastric leaks (1-2%), typically occurring several days after surgery and mostly located near the GE junction. Most leaks are now treated with endoscopically placed fully covered nitinol stents, left in place for several weeks, and abscess drainage. GERD reflux is improved in 80% of patients, but in some it may remain or worsen and require prolonged medical therapy or conversion to Roux-en-Y gastric bypass. (4) Weight loss failures can be treated with a variety of surgical options including re-sleeve gastrectomy, conversion to Roux-en-Y gastric bypass or duodenal switch. (5,6). Appropriate patient selection is important.
Need more information about surgeries?
For more information about our you can contact us and get more details.